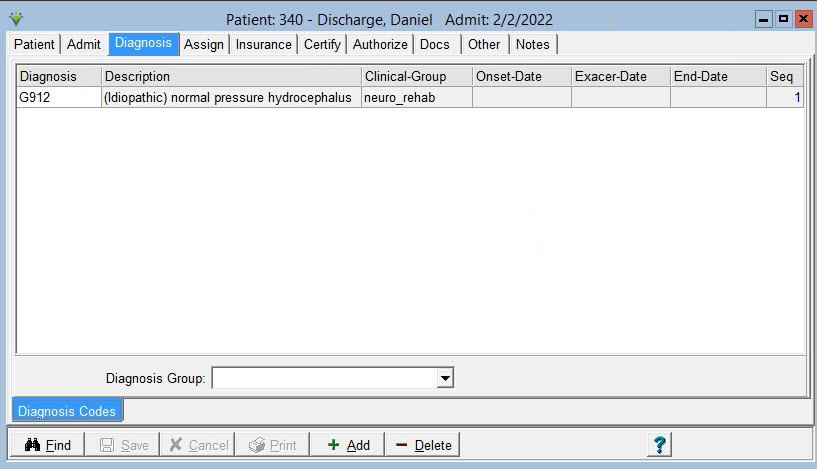
Adding/Maintaining Diagnosis Codes:
Press the  button to add the record.
button to add the record.
Click
on the drop-down list in the “Diagnosis” or “Description” fields, or
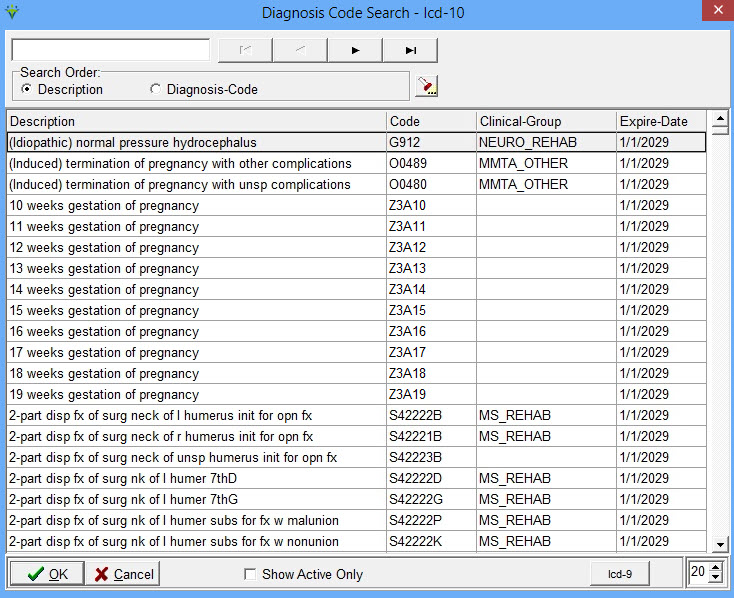
click on the Find button to select the Diagnosis. Press the "ICD10" or
"ICD9" button in the Diagnosis Search window to toggle between ICD10
and ICD9 code sets.
Onset-Date: Enter the Date the patient was diagnosed with
that condition, if known.
Exacer-Date: Enter the date of exacerbation for that
diagnosis
End-Date: Enter the date that condition ended for the
patient:
**Note: Usually only current diagnoses are stored on this
tab. The 485 Plan of Treatments will store the historical diagnoses.
Seq: Enter the sequence order the codes should appear in
patient documentation.
Diagnosis
Group: Select a Diagnosis Group if needing to run reports based
on diagnosis grouping. Typically only needed for reporting for
certain States such as NY State Report.
 : Click this button to check for any diagnosis code combinations that
can not be billed together per CMS's Excludes1 list in the diagnosis
code table they distribute.
: Click this button to check for any diagnosis code combinations that
can not be billed together per CMS's Excludes1 list in the diagnosis
code table they distribute.